22/F on OCPs and recent history of prolonged air travel. She was found to have a DVT and was started on Rivaroxaban a week ago. She presented to the ED with c/o Sudden onset chest pain, pre-syncope and SOB. With a clot in her legs, her story was certainly concerning a PE. These were her Vitals on arrival:
PR 128/min, BP 110/70, RR 28/min, SPO2 99% on Room Air
ECG - Sinus Tachy
PaO2 - 14kP (105mmHg)

I booked her for a CTPA on arrival since she was high-risk so d-dimer was not needed. Over the next hour, with some IV Fluids, her vitals settled down and looked a bit better.
PR 110/min BP 120/68 RR 24/min SPO2 99% Room Air
This made me wonder if a scan was really needed for her? Anyways, she was already on oral anticoagulation. Would I be able to justify myself for not doing a CTPA with textbook presentation of PE?
I ended up scanning her and she was found to have sub-segmental PEs. You might argue against a CTPA for this patient but her presentation and initial vitals kept me on my toes.
My learning points from this case:


Summary:
Further Reading

PR 128/min, BP 110/70, RR 28/min, SPO2 99% on Room Air
ECG - Sinus Tachy
PaO2 - 14kP (105mmHg)

I booked her for a CTPA on arrival since she was high-risk so d-dimer was not needed. Over the next hour, with some IV Fluids, her vitals settled down and looked a bit better.
PR 110/min BP 120/68 RR 24/min SPO2 99% Room Air
This made me wonder if a scan was really needed for her? Anyways, she was already on oral anticoagulation. Would I be able to justify myself for not doing a CTPA with textbook presentation of PE?
I ended up scanning her and she was found to have sub-segmental PEs. You might argue against a CTPA for this patient but her presentation and initial vitals kept me on my toes.
My learning points from this case:
- Normalization of initially abnormal vital signs should not be relied upon to r/o PE
- ABG and pulse oximetry do not reliably predict the presence or absence of PE
When should we start a working up PE?
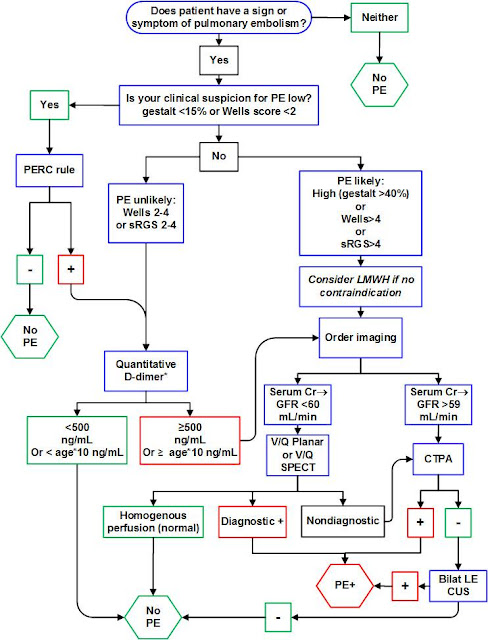
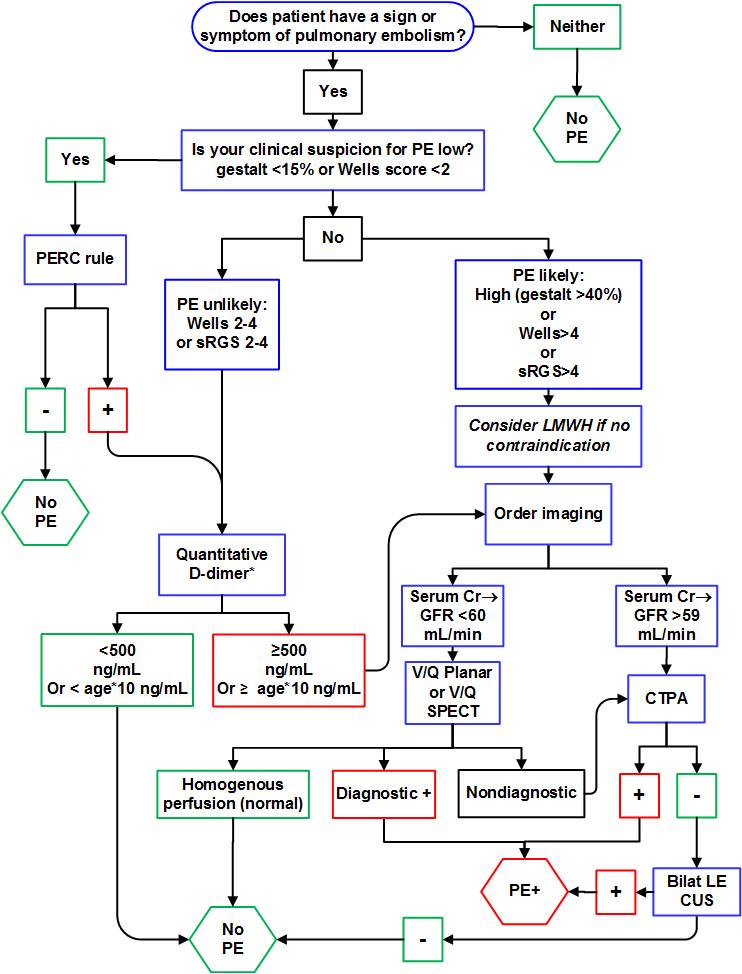
Start work up for PE if patient has any sign (Unexplained tachycardia/tachypnea, low SpO2) or symptom (Chest Pain, SOB) of PE. It is reasonable to consider PE as a differential when ECG shows evidence of right Heart Strain (S1Q3T3, Simultaneous TWI in inferior an pre-cordial leads).
Caveat: All patients coming with Chest pain do not need a work up for PE. Risk Stratify them and score them on Well's criteria and PERC rule before starting the work up. Random ordering of d-dimer leads to false positive and unnecessary imaging/anticoagulation.
Random d-dimer sent on a patient with Non-Specific Chest Pain. Can't we just ignore that?
D-Dimer is a great test if used sensibly. It is reassuring if negative (in low risk patients) to exclude PE. Always utilise d-dimer with clinical probability.

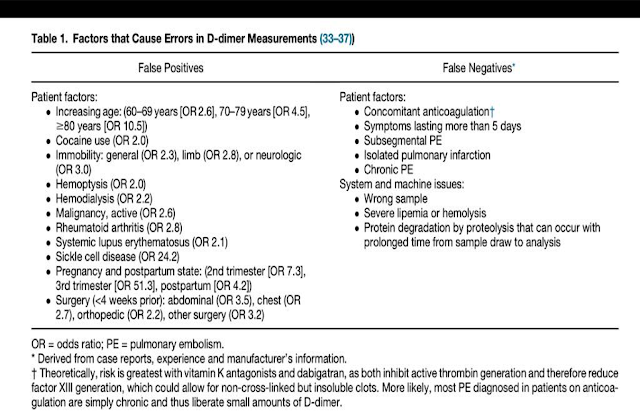
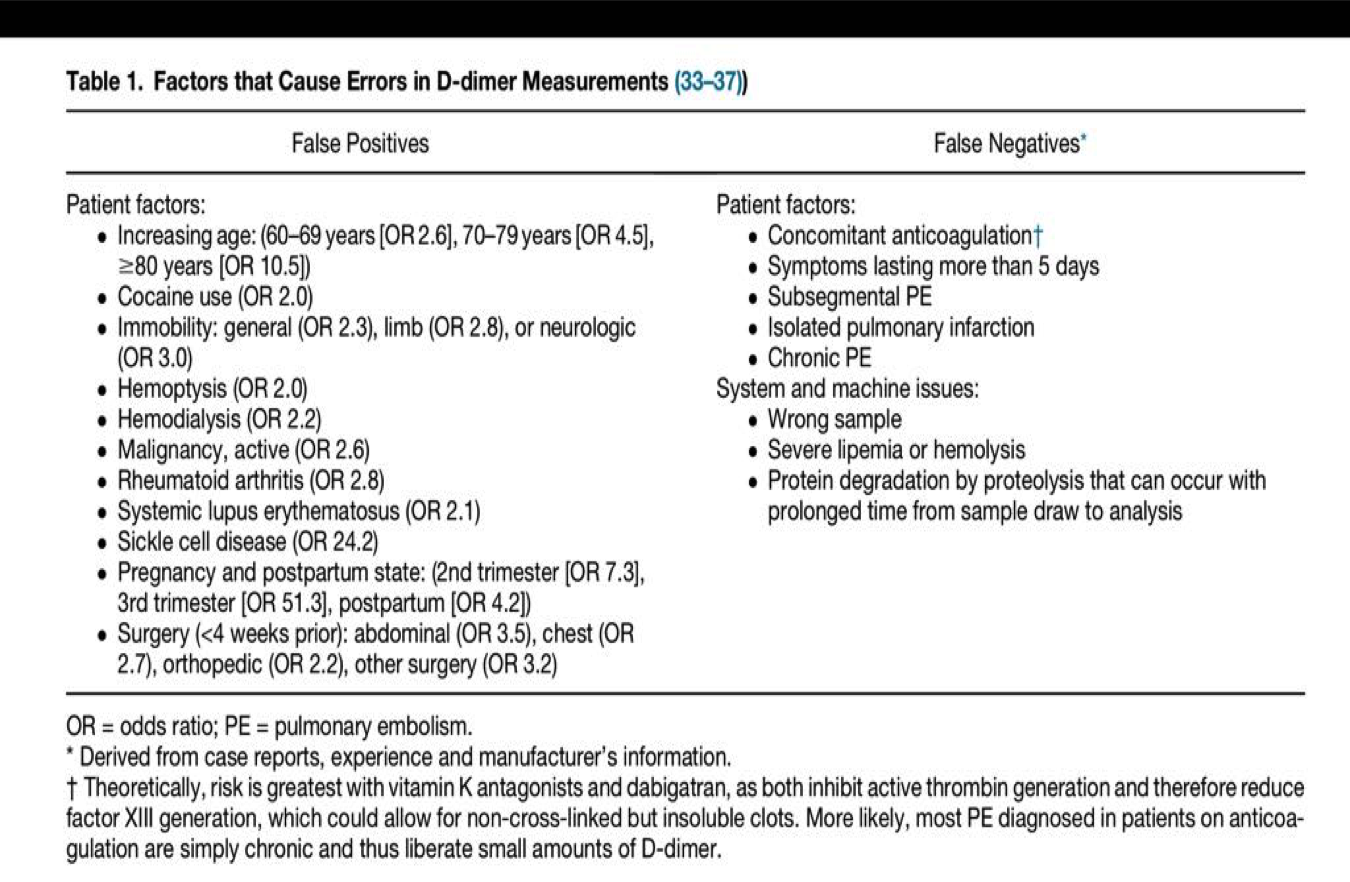
If you are thinking high risk for PE, do not even bother sending a d-dimer. You will need imaging to rule out PE in high-risk regardless of the d-dimer results. As with every test in medicine, there are false positives and false negatives with d-dimer as well. We often talk about the non-specificity of d-dimer and false positives. Here is a list of things that cause false positive and false negative d-dimer.
Of course, you can disregard an elevated d-dimer but you should have a reasonable explanation for that. It should be documented clearly why imaging (CTPA or VQ) was not pursued if d-dimer was found elevated.
When do we consider thrombolysis for PE?
PEs can be classified as:
- Massive PE is defined as acute PE with obstructive shock or SBP <90 mmHg
- Submassive PE is acute PE without systemic hypotension (SBP ≥90 mm Hg) but with either RV dysfunction or myocardial necrosis (positive troponin or ECHO evidence of RV dysfunction)
- Low risk PEs
Click here to read more about thrombolysis in PE.
Troponin is not helpful in the diagnosis
of PE, but it is helpful in the assessment for severity of disease.
Do we
need to treat small distal clots but without DVT (single clot <3mm)?
Isolated distal clots can represent a possible artefact
rather than true disease. Many Sub segmental PEs are not even seen by another radiologist when blinded. But guidelines still recommend to treat if risk factors present or if symptomatic and has low risk of bleeding.
What if CTPA turns negative but you have extremely high suspicion for PE?
Ask
radiologist about the quality of scanner. Clinical context holds above everything else. Remember,
Gold Standard for diagnosis is Pulmonary Angiography.


When
to consider IVC filter, cather
directed lysis?
The indications for IVC filter include:
(1) Patients with contraindications to anticoagulation
(2) Those who have complications from the use of anti-coagulation
(3) Those who fail to attain adequate anticoagulation while undergoing treatment.

Cather directed lysis should be first line if available for massive PE.
(1) Patients with contraindications to anticoagulation
(2) Those who have complications from the use of anti-coagulation
(3) Those who fail to attain adequate anticoagulation while undergoing treatment.

Cather directed lysis should be first line if available for massive PE.
Working
up PE in pregnancy?
Start with lower extremity doppler (if DVT+ and hemodynamically stable, start anti-coagulation). Some authorities do not even recommend sending a d-dimer in pregnancy while others recommend using trimester adjusted d-dimer. When used in pregnancy, d-dimer can be extremely helpful when negative. Here is an algorithm based on using trimester adjusted d-dimer.

If you do not want to use d-dimer at all then you have these options:
- Treat with Heparin Doppler if positive for DVT
- ECHO/Troponin to further risk stratify
- CTPA (Radiation is 4 times more than that of a V/Q scan)
- VQ Scan (done only if CXR is normal, if CXR abnormal then go for CTPA)
CTPA - Good for baby, Bad for Mom
V/Q - Bad for baby, Good for Mom

Consider V/Q in cases of Allergy
to iodine contrast, Impaired
Renal Function and Pregnancy. Issues with V/Q scan can be availability, expertise to interpret the scan. V/Q often gets interpreted as low probability or intermediate probability which leaves you nowhere!
Too many CTPAs can give you false positives and lead to over-diagnosis and over treatment. Ask yourself, if that tiny clot is really responsible for your patient's symptoms or was it just an incidetaloma!
The least desirable scenario
is one in which both a V/Q scan and a CTPA are
needed to complete the diagnostic evaluation.
Working up PE in a patient already on oral anticoagulants?
Anticoagulants
can make d-dimer unreliable and there is no
clear consensus on this.
CTPA them if you have any concerns for a PE and plan for an IVC filter if they are CTPA positive.

Consider targeting higher INR as they are throwing clots even on oral anti-coagulants.

Consider targeting higher INR as they are throwing clots even on oral anti-coagulants.
Summary:
The testing to catch Pulmonary Embolisms has skyrocketed over the last decade. The
increased use of CT in patients with suspected PE
has resulted in an increase in the diagnosis of PE but
without an associated mortality benefit. Start a work up for PE based on your gestalt or Well's Criteria followed by PERC rule (Low risk on Well's Criteria and PERC negative does not even need a d-dimer). Every test comes with caveats (d-dimer, CTPA, VQ scan) and we must act in a prudent manner while ordering imaging to avoid unnecessary anti-coagulation.
Further Reading
- Age-Adjusted d-dimer
- Tichauer M. The Emergency Medicine Approach To The Evaluation And Treatment Of Pulmonary Embolism. Emergency Medicine Practice. 2012:2.
- Kline JA, Kabrhel C. Emergency evaluation for pulmonary embolism, Part 2: diagnostic approach. The Journal of emergency medicine. 2015 Jul 31;49(1):104-17.
Posted by:
Lakshay Chanana
Speciality Doctor
Northwick Park Hospital
Department of Emergency Medicine
England
No comments:
Post a Comment